Knocked Out a Tooth Playing Soccer? What to Do in the Next 60 Minutes.

World Cup season brings something out in everyone — the games, the energy, the pickup matches in the backyard and the park. And every year around this time, we see a predictable uptick in dental trauma. Kids and teenagers especially, playing harder and faster than usual, sometimes at the cost of a tooth.
A knocked-out tooth is one of the most time-sensitive dental emergencies there is. What you do in the first 30 to 60 minutes — and what you don't do — directly determines whether that tooth can be saved.
This post is short, practical, and worth reading before you need it.
The Golden Window: 30 to 60 Minutes
When a permanent tooth is completely knocked out — the clinical term is avulsion — the clock starts immediately. The tooth's root surface is covered in periodontal ligament cells: living tissue that, under the right conditions, can reattach to the socket. These cells begin dying within minutes of drying out.
Within 30 minutes: Reimplantation success rates are high. The periodontal ligament cells are still largely viable, and with proper handling, the tooth has a strong chance of reattaching.
30–60 minutes: Success rates decline but remain meaningful. Getting to a dentist in this window is still worth every effort.
Beyond 60 minutes: The prognosis changes significantly. Reimplantation may still be attempted, but long-term survival of the tooth becomes considerably less certain.
Time is the variable you can control. Everything else follows from that.
What to Do — Step by Step
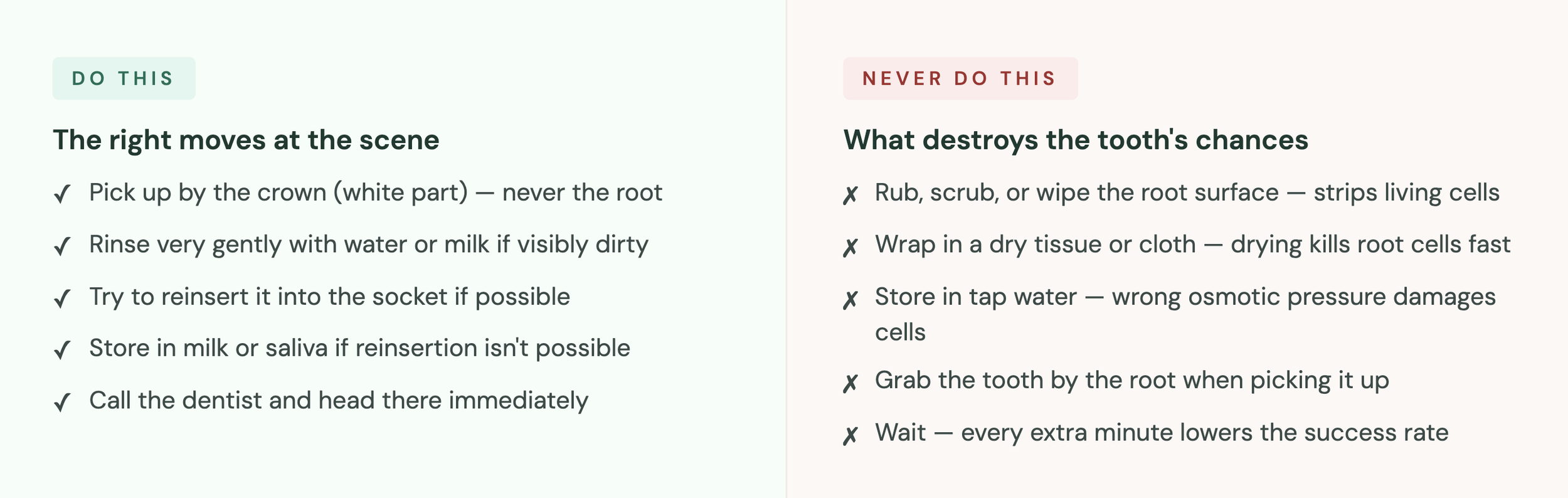
Step 1: Pick up the tooth by the crown, not the root. The crown is the white part you normally see in the mouth. The root is what goes into the gum. The root surface contains those critical periodontal ligament cells — handling it roughly, or touching it at all more than necessary, damages them. Pick the tooth up carefully by the crown only.
Step 2: Do not rub, scrub, or wipe the tooth. This is the most common mistake made at the scene, usually with the best intentions — someone grabs a shirt or tissue to "clean" the tooth. Don't. Even gentle wiping strips away the periodontal ligament cells on the root surface. If there's visible dirt, rinse very gently with clean water or milk. No scrubbing, no soap, no rubbing.
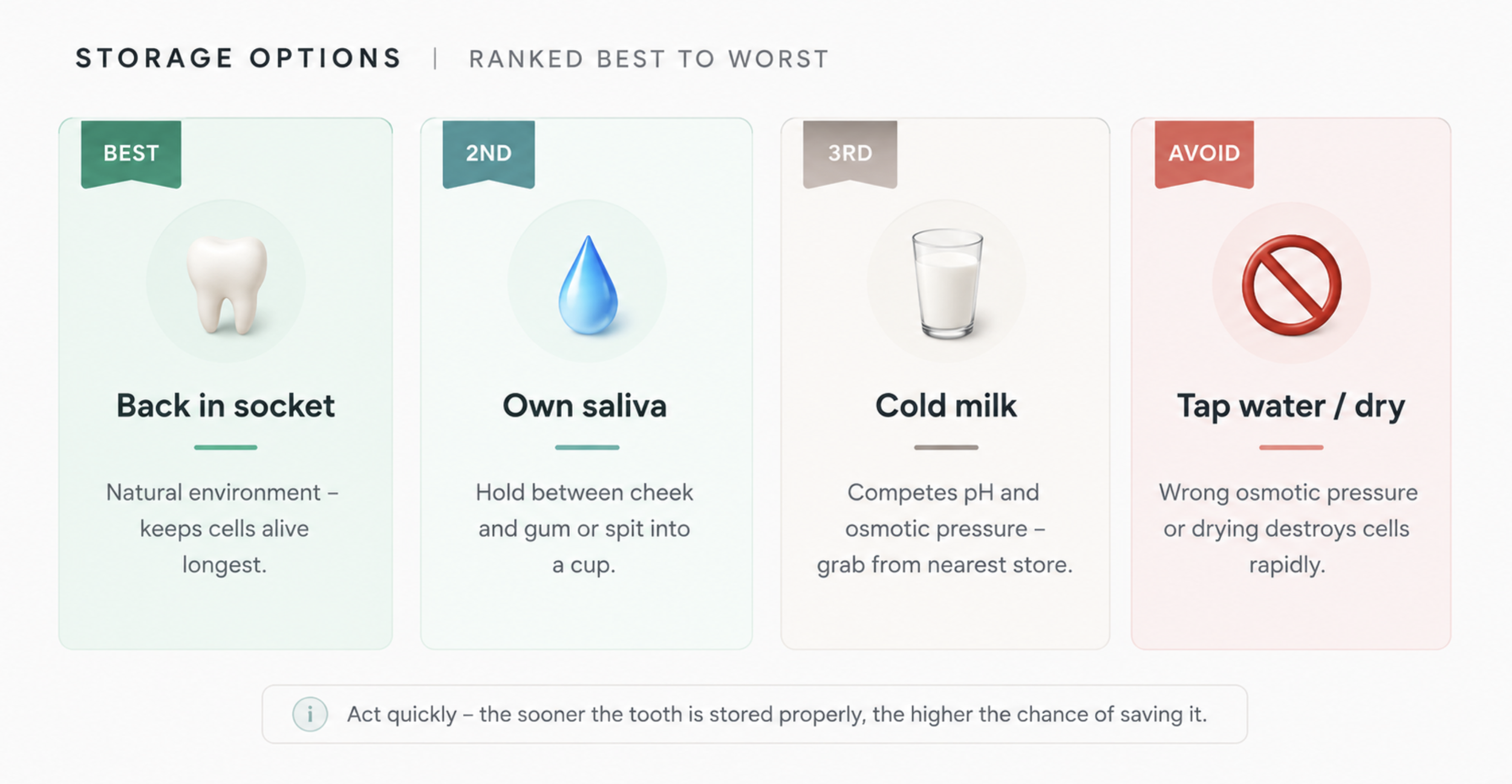
Step 3: Try to reinsert it. If the patient is calm enough and old enough to follow instructions, the best storage for a knocked-out tooth is back in its socket. Rinse gently, orient the tooth correctly (smooth side facing out), and press it back into place with steady, gentle pressure. Have the patient bite down softly on a clean cloth to hold it in position. This keeps the root cells alive in their natural environment.
Step 4: If reinsertion isn't possible, store it correctly. If the tooth can't be reinserted — because of the patient's age, distress, or injury — storage medium matters enormously.
Best: The patient's own saliva. Have them hold the tooth between their cheek and gum, or spit into a small container and store the tooth in it. Saliva maintains the right osmotic environment for the cells.
Second best: Cold milk. Milk has a compatible osmotic pressure and pH for periodontal ligament cell survival. This is the go-to recommendation when saliva isn't practical — a cup of cold milk from a nearby store buys meaningful time.
Third option: Saline (contact lens solution). If available, sterile saline works. Regular tap water is not recommended — its osmotic pressure causes cell swelling and death relatively quickly.
Do not store dry. A tooth sitting on a paper towel or in a pocket dries out rapidly. Dry storage is the fastest way to lose viability.
Step 5: Get to a dentist immediately. Call ahead if you can — we'll prepare for your arrival. Do not stop at urgent care unless no dental option is available. Reimplantation requires dental expertise, and the faster you arrive, the more we can do.
What About a Chipped or Fractured Tooth?
Not every dental trauma involves a completely knocked-out tooth. Chips and fractures are more common, and the urgency level varies with severity.
Minor chip (enamel only): Not a same-day emergency, but should be evaluated within a day or two. Rough enamel edges can irritate soft tissue, and the tooth needs assessment to rule out deeper damage.
Moderate fracture (into dentin): Sensitivity to air, temperature, or touch indicates the fracture has reached the dentin layer. This should be seen the same day or within 24 hours. The tooth needs protection to prevent further exposure or bacterial entry.
Severe fracture (reaching the pulp): If you can see pink or red tissue in the fracture, or the patient has significant pain, this is an urgent emergency. The nerve is exposed. Same-day care is essential.
Root fracture: These don't always cause obvious pain but require prompt evaluation. If a tooth feels loose after impact, even without visible damage, it needs to be checked.
The general rule: when in doubt, come in. Dental trauma that appears minor can involve damage that isn't visible without examination and X-rays.
A Note About Mouthguards
Since we're talking about soccer and World Cup season — this is worth saying directly.
Custom-fitted mouthguards are the most effective way to prevent dental trauma during contact and collision sports. Studies consistently show they reduce the risk of tooth injury by a significant margin. The boil-and-bite versions from sporting goods stores provide some protection, but fit less precisely and offer less coverage than a professionally made guard.
If your child plays soccer, football, basketball, martial arts, or any sport with collision risk — a custom mouthguard is a reasonable investment. One dental trauma event costs more in time, treatment, and anxiety than a mouthguard ever will.
We can make one at a regular appointment. It takes one impression and about a week.
Frequently Asked Questions
Can a knocked-out permanent tooth be saved? Yes — if handled correctly and seen within the golden window of 30 to 60 minutes, reimplantation has a meaningful success rate. The key variables are time, storage, and how the tooth is handled before arrival.
What should I store a knocked-out tooth in? In order of preference: back in the socket (best), in the patient's own saliva, in cold milk, or in sterile saline. Avoid tap water and dry storage — both damage the root cells quickly.
What if it's a baby tooth? Baby teeth are generally not reimplanted — attempting to force them back in can damage the developing permanent tooth underneath. Bring the child and the tooth to the dentist, but do not try to reinsert it yourself.
Does this apply to kids and adults equally? The same principles apply to both, but timing is equally critical. The golden window doesn't expand for adults — if anything, the stakes are higher because there's no permanent replacement waiting.
What if I can't get to a dentist immediately? Keep the tooth in milk or saliva, minimize handling, and get to an emergency dental provider as fast as possible. If it's after hours, call our office — we have an emergency line.
The Thing About Dental Emergencies

They never happen at a convenient time. They happen at the soccer tournament, during the World Cup viewing party, on a Saturday afternoon when no one's thinking about teeth.
The difference between a tooth that gets saved and one that doesn't is almost never about the severity of the injury. It's almost always about what happened in the first hour — and whether someone nearby knew what to do.
Save this post. Screenshot it. Send it to the group chat before the tournament weekend.
And if it happens to you or someone you love, call us immediately.
📍 State Avenue Dental Office — Kansas City, KS (KCK) 🗣 English • Korean • Spanish